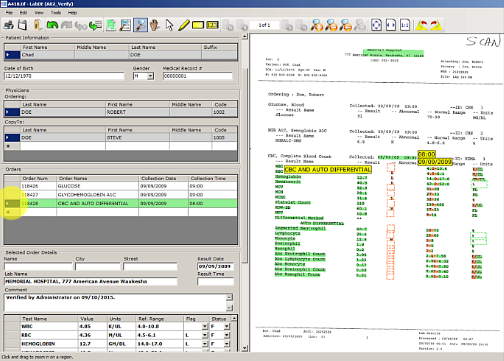
In a recent Health Informatics Journal article reporting of “true integration” of electronic laboratory results, it was mentioned that transcription errors remain a bottleneck with comprehensive electronic health records. This shouldn’t come as a surprise to those who encounter paper labs every day in their daily workflow. For most hospitals, a significant number of records are interfaced. But if you are working with paper daily, you might think it debatable that manual data entry is insignificant.
These days, clinical informatics departments are working hard to solve many priority issues. But depending on where your hospital is located geographically, your clinical information challenges have a direct correlation with the patient population your hospital is serving. For example, if your patients travel very long distances to your facility, it is very likely that your clinical services are handling and entering results from paper labs and dealing with costly transcription errors.
Similarly, if you are like most organizations, you
Read More