Posted by
David Rasmussen
on Jun 23, 2016 9:30:00 AM
Shocking? Yes. New? Not even close.
The headline Medical Errors are the Third Leading Cause of Death is a popular title for a recent study that highlights the impact diagnostic errors can have on patients.
A web search turned up similar headlines every few years going back to the 1990’s. Clearly, not much has changed. There are still too many diagnostic errors and not enough has been done to reduce the carnage.
Read More
Posted by
Dr. John Daller, MD, PhD, FACS
on Jun 21, 2016 9:30:00 AM
What Are Objective Measures and How Do I Start to Pick Them
In our first blog of this series, we discussed the model framework for developing a Quality Assessment Process Improvement program. Today, we will discuss how to develop objective measures that are used in three of the aspects of the program, namely Feedback, Data Systems and Monitoring; Systematic Analysis and Systemic Action; and Performance Improvements. The directive to employ objective measures is provided in the Centers for Medicare and Medicaid Services (CMS) Conditions of Participation (§482.96(a) Standard: Components of a QAPI Program) that states: “The transplant center’s QAPI program must use objective measures to evaluate the center’s performance with regard to transplantation activities and outcomes”. These objective measures must be in each phase of transplantation (pre-transplant, transplant and post-transplant) as well as donation (pre-donation, donation and post-donation).
Read More
Posted by
Dr. John Daller, MD, PhD, FACS
on Jun 14, 2016 3:41:40 PM
In our previous blogs, we have reviewed some aspects of transplant operations, how to stay compliant and how to address concerns raised by regulatory agencies such as the United Network for Organ Sharing (UNOS) and the Centers for Medicare and Medicaid Services (CMS) when issues arise. Our next series of blogs will focus on how transplant programs can proactively track their progress and address potential problems before they become major issues. During this series, we will review the structure, operations and tools of an effective Quality Assessment and Process Improvement Program (QAPI). First, let’s review the 5 aspects that create the conceptual framework for a QAPI program under the Medicare requirements.
Read More
Posted by
Rob Fea
on Jun 13, 2016 9:00:00 AM
Once again I had the pleasure of attending the 24th Annual UNOS Transplant Management Forum for my 4th time earlier this year. As always, it was a flurry of learning, knowledge-sharing, networking, and well-deserved awards for leaders in the industry.
Read More
Posted by
Greg Gies
on Apr 30, 2016 10:10:00 AM
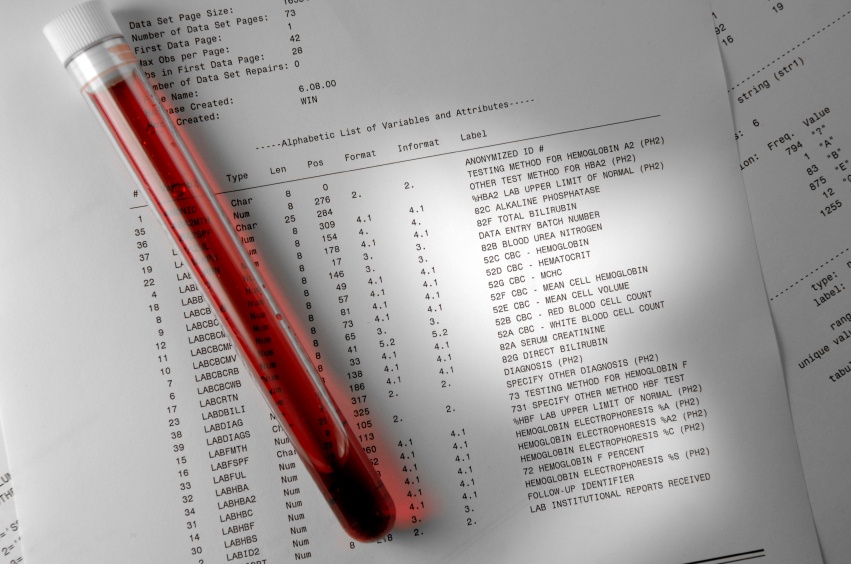
Spend more time finding a cure and less time finding and redacting PHI.
Preparing patient records for research analysis is a painstakingly laborious process. De-identifying records is the main culprit. Manual point-and-click redaction tools are no match for large-scale jobs involving complex patient records.
Read More
Posted by
Greg Gies
on Apr 30, 2016 9:48:00 AM
Your incomplete data set doesn’t tell you the full story.
 A population health management program without the ability to analyze a complete set of clinical data is like reading a book with missing pages. You’re left with only your imagination to fill in important details.
A population health management program without the ability to analyze a complete set of clinical data is like reading a book with missing pages. You’re left with only your imagination to fill in important details.
Read More
Posted by
Greg Gies
on Apr 30, 2016 9:31:00 AM
Clinical labs should be tests for your patients, not a test of your patience.
Delivering high quality care in a timely manner is the best way to ensure patient safety and satisfaction. Clinical labs are often a critical step on the path to diagnosis and treatment. Test results from outside labs are often delayed or hard to find amid a sea of PDF files in the EHR, or worse, in a pile of paper faxes.
Read More
Posted by
Greg Gies
on Apr 30, 2016 9:20:00 AM
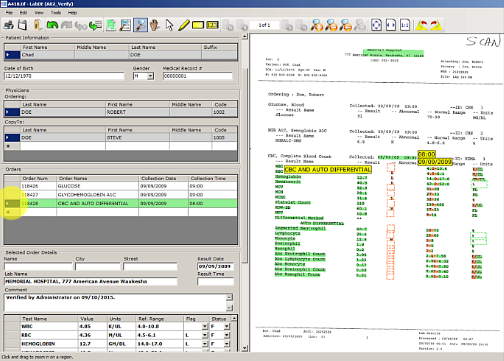
No interface? No problem. Automatically capture send-out test results into your LIS.
Unfortunately, setting up lab interfaces to every reference lab isn’t an option. This is especially true for low volume, high value esoteric labs.
Consequently, communications of test results are delayed while test data is keyed in. Manually keying test results in the LIS is slow, error-prone and, when done correctly with redundant data entry, imposes a high opportunity cost.
Read More
Posted by
Chantel Soumis
on Apr 30, 2016 8:58:00 AM
Stop digging through PDF attachments in your EHR media tab.
For clinicians, finding test results in the EHR can feel like an archeological dig – except it’s not as fun.
Too often the complete patient story is buried deep within unstructured document attachments, such as scanned copies of faxed test results.
Read More
Posted by
Greg Gies
on Apr 30, 2016 6:00:00 AM
Only meeting the minimum MU2 core measure for labs compromises clinical decisions costing $317,178 per bed each year.
Meaningful Use Stage II core measure for lab results requires that lab values are captured in structured EHR data fields for only 55% of results. That means as many as 45% of decisions informed by test results that aren’t easily accessible or trendabale -- driving up the cost of care and compromising care quality.
Read More