Greg Gies
For 20 years in the software industry, Greg Gies has been helping businesses, government agencies and healthcare organizations achieve their goals and carry out their missions by making better use of information and automating business processes. Greg has held positions in sales, product management and marketing and holds an MBA from Babson College. He works and lives with his wife and three boys in the Boston area. You can read more of Greg’s blog posts here and connect with Greg on LinkedIn.
Posted by
Greg Gies
on Oct 19, 2015 4:44:51 PM
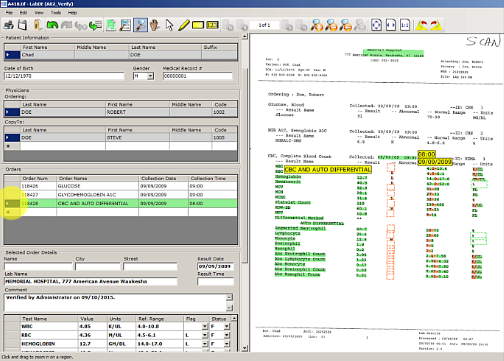
Lab tests are one of the highest volume activities in healthcare that inform between 70 - 80% of all clinical decisions. Keeping pace with the high volume of lab results that are so vital to patient care can at times be overwhelming. Complicating matters more are the lab results that don’t come “over the wire” via an electronic lab interface– what are often referred to as non-interfaced or external lab results. The challenge gets even more complicated when you receive partial or duplicate lab results from non-interfaced sources.
Read More
Posted by
Greg Gies
on Oct 13, 2015 8:00:00 AM
If you’re responsible for managing the process or technology for relaying test results from reference labs to ordering physicians, you’re probably familiar with the difficulty of handling non-interfaced clinical lab results even if you’re not familiar with the term “non-interfaced.”
Simply stated, non-interfaced lab results are diagnostic test reports that arrive by mail, are carried in by a patient, arrive on your fax machine, fax server inbox or that you download from a portal instead of results that are transmitted to your office through lab interfaces.
Read More
Posted by
Greg Gies
on Oct 5, 2015 5:38:00 PM
Last week I published the second in a series of seven blog posts that discuss some of the misperceptions about lab interfaces and intelligent clinical data extraction software.
Below is the list of misperceptions this blog series will cover in the span of seven weeks. This post addresses the second misperception in bold type in the list below.
- We are implementing or already have an interface to Quest and/or Labcorp and no longer have to manually enter test results.
Read More
Posted by
Greg Gies
on Sep 24, 2015 6:24:03 PM
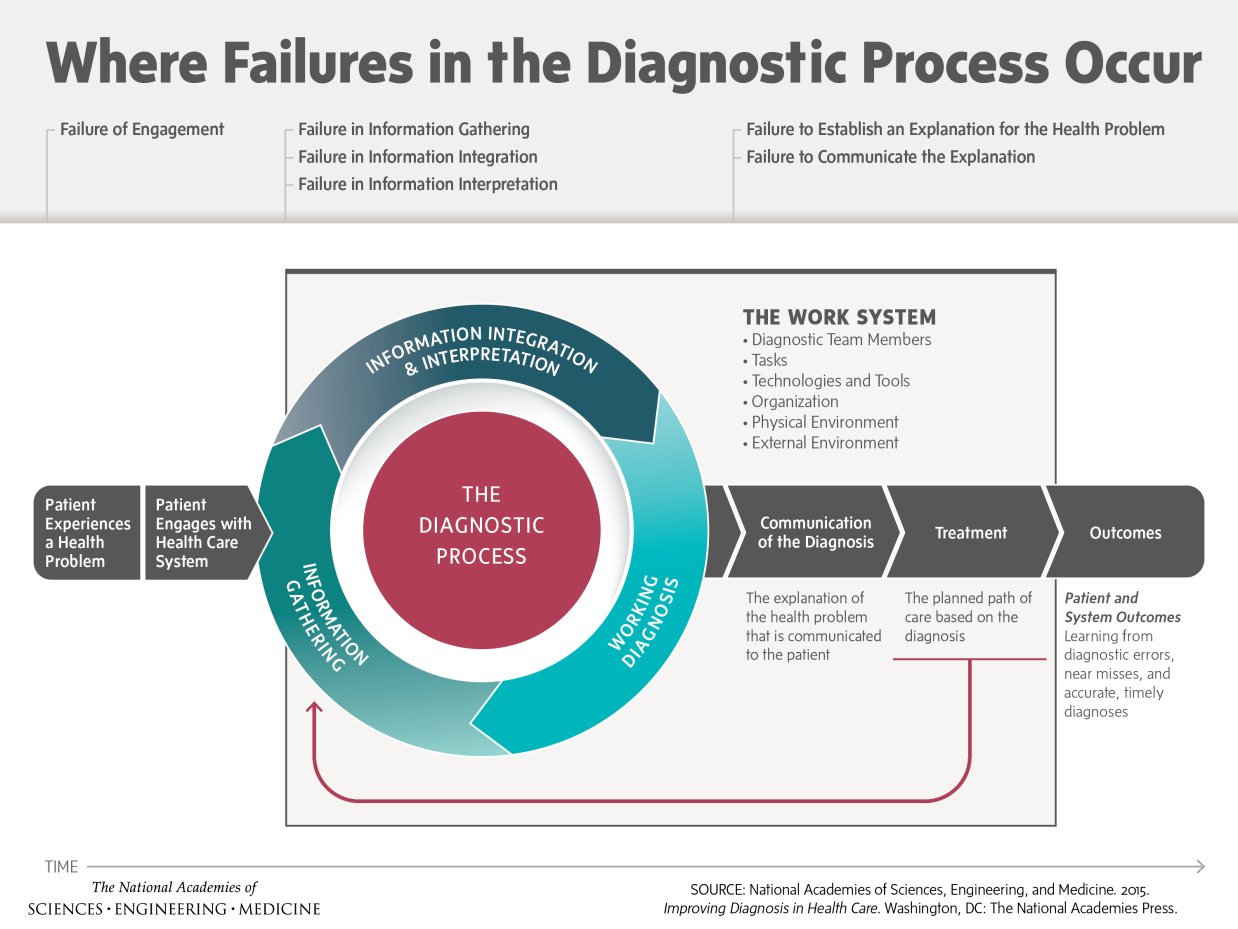
Yesterday, the prestigious Institute of Medicine (IOM) announced a soon-to-be-released report highlighting diagnostic errors as a persistent “blind spot in the delivery of quality health care” and urges the healthcare industry to change in order to address the prevalence of diagnostic errors, which the IOM defines as “the failure to (a) establish an accurate and timely explanation of the patient’s health problem(s) or (b) communicate that explanation to the patient.”
The report synopsis available on the IOM website identifies several failure points in the clinical diagnostic process. Not surprisingly, it identifies information integration as a one of those failure points.
Read More
Posted by
Greg Gies
on Sep 15, 2015 4:01:45 PM
Almost 50 percent of hospitals with 200 or more beds will purchase a new electronic medical record system by 2016, according to a KLAS report. Even after sizable investments in new EMRs that meet meaninful use guidelines, complete and accurate patient information available to physicians, much less the enterprise, remains elusive.
Read More
Posted by
Greg Gies
on Aug 21, 2015 10:22:41 AM
Last week I published the first in a series of seven blog posts that discuss some of the misperceptions about lab interfaces and intelligent clinical data extraction software.
Read More
Posted by
Greg Gies
on Aug 18, 2015 8:22:00 PM
As I’m standing in line at my favorite coffee shop, I’m thinking about how baristas have perfected workflow; and now have improved perfection by allowing me to eliminate the line entirely by ordering in advance with my smart phone. It always excites me when I see a sequence of steps refined for optimum efficiency. I know it's odd, but I'm really strange like that.
Read More
Posted by
Greg Gies
on Aug 13, 2015 11:35:00 AM
In the course of helping hospitals automate data entry of clinical lab results into the EMR (or LIS in cases where all orders are centrally managed) we’ve spoken to thousands of healthcare professionals about their
lab results reporting procedures. Invariably the subject of “lab interfaces” comes up. There are several misperceptions about interfaces and intelligent clinical data extraction software and lab results interoperability in general that I’ll attempt to clear up in a series of seven blog posts.
Read More
Posted by
Greg Gies
on Aug 3, 2015 11:52:00 AM
In an article in Forbes business magazine today, Peter Ubel, begins to investigate the question of whether or not we should be striving for a world in which all transplant candidates should have access to LearJets so that they can place themselves on multiple waiting lists and have a greater chance of reaching the top of that list in time? No matter how you feel personally or professionally about this issue, an important point that he raises in the world of transplant is this: as technology (planes, drugs, etc.) improves and allows for greater possibilities of organs for a greater pool of candidates, how can we be sure that waitlists are always accurate and up to date. What technologies do we need to deploy to be sure that they are so that we can keep up with the speed in which patients can be ushered to us? Being certain that all the data you need in order to maintain these waitlists are accurate and ready to compute the items needed to update that list are very important. If you have lab results or other important documents in a pile of documents, can you be sure you have the most accurate list?
Read More
Posted by
Greg Gies
on Aug 3, 2015 8:09:00 AM
Recently, I had the misfortune of sustaining an injury while running. Due to the nature of my injury I visited a total of five providers in the span of one week. The events that unfolded provided the perfect opportunity to reflect on the state of health information interoperability six years after the passing of the HITECH Act.
Read More